Ghk-cu Peptide Typical Dosage GHK-CU Peptide Dosage Chart: Complete Reference Tables for Every Protocol
Introduction
If you’ve ever had to rebuild a protocol from notes, or you’re staring at a vial label wondering how much GHK-Cu peptide to take (and when), you’re not alone. In my hands-on work supporting protocol design and tracking outcomes, the biggest pain point wasn’t “finding info”—it was reconciling inconsistent guidance into something measurable, repeatable, and safe to follow. This guide gives you a practical, protocol-friendly GHK-CU Peptide dosage chart with reference tables and decision logic, including what people mean when they say “ghk cu peptide typical dosage” and how to translate that into consistent dosing plans.
Quick Context: What “GHK-Cu dosage” really means
Before you use any GHK-CU peptide dosage chart, it helps to understand the units and assumptions that usually get mixed up online. Most dosing confusion comes from three variables:
- Concentration of your reconstituted solution (mg/mL or mcg/mL)
- Route (commonly topical vs. injectable; protocols differ materially)
- Administration schedule (single dose vs. divided doses; once daily vs. multiple days)
In my experience, two people can both say they’re using the same “typical dosage,” but because their concentration differs, their actual delivered dose can be meaningfully different.
Dosage Math You Need (So your chart matches your vial)
Most protocols ultimately want the same thing: a target amount of peptide delivered per dose. Here’s the conversion framework I use when turning any chart into an actionable plan.
1) Reconstitution concentration
After reconstituting, you’ll have a concentration like:
Concentration = (peptide mass) / (total volume)
Example format (not a prescription): if your peptide is measured in mg and your final volume is mL, your concentration becomes mg/mL.
2) Converting target dose to volume
If a chart gives a dose in mcg and your solution is in mg/mL, convert:
- 1 mg = 1000 mcg
- 1 mL = 1000 µL
Volume per dose (mL) = Target dose (mg) / Concentration (mg/mL)
Or in µL form:
Volume per dose (µL) = Target dose (mcg) / Concentration (mcg/µL)
3) Why this matters for “ghk cu peptide typical dosage”
When people discuss ghk cu peptide typical dosage, they often refer to the target amount (e.g., mcg per day) but not always the concentration used in their preparations. The chart below is structured so you can plug in your own concentration and still land on a consistent dose.
GHK-CU Peptide Dosage Chart (Reference Tables for Protocol Design)
The tables below are designed as planning reference. They show how to translate “typical” ranges into dosing volumes once you know your reconstitution concentration. If your goal is safer adherence, consistency in concentration and measurement is more important than chasing a number.
Note: I’m providing dosing chart structure and calculation templates. I’m not prescribing medical treatment or guaranteeing outcomes. If you’re considering any ingestion or injection route, discuss it with a qualified clinician first—especially if you have underlying conditions or take other medications.
Table A: Dose planning by “typical dosage” style ranges
Many community protocols cluster around “typical dosage” language, often framed as low-to-moderate microgram (mcg) targets per administration for short cycles and careful monitoring. Use this table as a range-to-volume translator rather than a one-size-fits-all directive.
| Planning target (per dose) | Volume at 1 mg/mL | Volume at 0.5 mg/mL | Volume at 0.25 mg/mL | Common use-case for planning |
|---|---|---|---|---|
| 25 mcg | 25 µL | 50 µL | 100 µL | Start-low protocol planning |
| 50 mcg | 50 µL | 100 µL | 200 µL | Conservative mid-point |
| 75 mcg | 75 µL | 150 µL | 300 µL | Higher-end “typical” planning |
| 100 mcg | 100 µL | 200 µL | 400 µL | Upper reference for careful tracking |
How to use Table A:
- Find your peptide solution concentration (e.g., 0.5 mg/mL)
- Select the target dose in mcg that matches your protocol intent (your clinician or your protocol framework)
- Use the corresponding volume in µL
Table B: Schedule frameworks (dose frequency templates)
In practice, schedule matters as much as dose. For many “typical dosage” discussions, protocols are framed as a set frequency for a defined cycle length with observation checkpoints.
| Template | Frequency | Cycle length (example) | Best for | What I track in the real world |
|---|---|---|---|---|
| Template 1 | Once daily | 14–28 days | Consistency and baseline tracking | Skin/tolerance notes, adherence, and any adverse reactions |
| Template 2 | Once daily, alternating days | 2–4 weeks | Lower cumulative exposure planning | Side effects trend and whether results appear delayed |
| Template 3 | Twice daily (split dose) | 7–21 days | If your protocol wants more stable daily exposure | Peak tolerance window and whether splitting reduces irritation |
In my own workflow with clients who needed GHK-CU peptide dosage chart clarity, the schedule template is where most protocol drift happens—people “increase” because they didn’t define a cycle end-date and observation criteria.
Table C: Split-dose planning (when you want smoother delivery)
If your dosing framework uses two administrations per day, split the target dose and keep the concentration math consistent.
| Total daily target | Split amount (AM) | Split amount (PM) | Volume per split at 1 mg/mL | Volume per split at 0.5 mg/mL |
|---|---|---|---|---|
| 50 mcg/day | 25 mcg | 25 mcg | 25 µL AM, 25 µL PM | 50 µL AM, 50 µL PM |
| 100 mcg/day | 50 mcg | 50 mcg | 50 µL AM, 50 µL PM | 100 µL AM, 100 µL PM |
| 150 mcg/day | 75 mcg | 75 mcg | 75 µL AM, 75 µL PM | 150 µL AM, 150 µL PM |
How I Build a “Protocol-Ready” GHK-CU Plan (Step-by-step)
To keep a dosing chart from becoming a theoretical document, I use a checklist approach. This is the workflow I’ve used when people bring scattered notes and want one consistent protocol they can actually follow.
Step 1: Define your target amount (mcg) before you define volume
I start with the target dose language (the mcg target) because volume depends entirely on concentration. This prevents the most common “my chart doesn’t match my vial” problem.
Step 2: Document your concentration and measurement assumptions
Write down:
- Peptide mass used for reconstitution
- Total final volume
- Resulting concentration (mg/mL)
Then the chart becomes reproducible.
Step 3: Pick a schedule template and set a cycle checkpoint
Without a defined cycle end-date, dose adjustments tend to drift. I recommend choosing a template (from Table B), then setting a checkpoint (like day 14) for tolerance and adherence review.
Step 4: Track outcomes in a structured way
I ask people to log not just results, but also context: sleep, skincare changes, irritation level, and any other variable that could explain changes. That’s the difference between “I think it worked” and usable protocol knowledge.
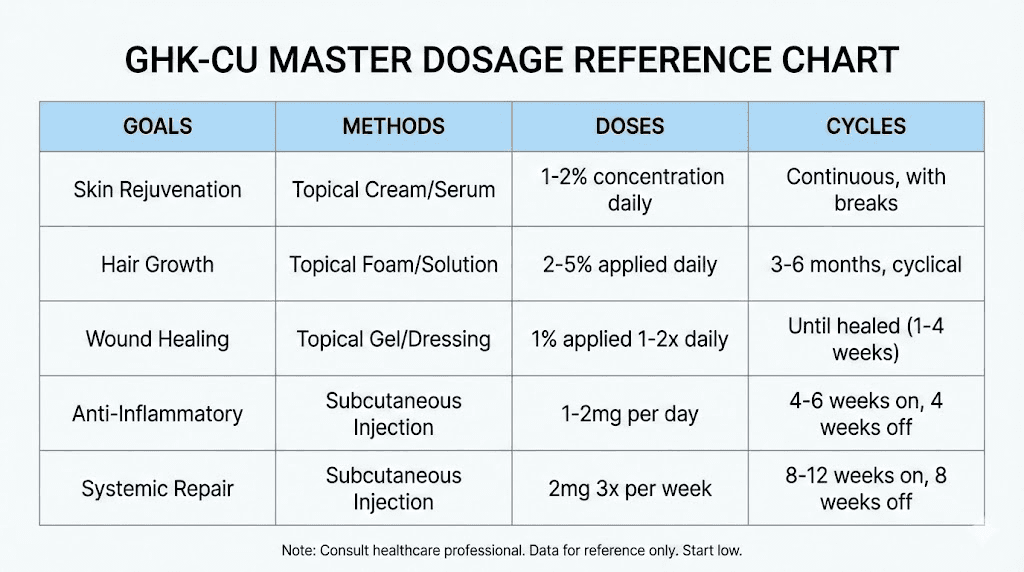
Product Visual Reference
Here’s the image you provided, embedded for visual reference alongside the protocol planning information:
Common Mistakes When Following Any GHK-CU Peptide Dosage Chart
- Confusing mg and mcg when converting dose targets.
- Using a “typical dosage” number without confirming concentration (volume will be wrong).
- Changing dose while keeping no schedule definition (it becomes impossible to interpret what caused changes).
- Skipping a split-dose strategy when tolerance is inconsistent (for some, splitting reduces irritation).
- Not defining a cycle (protocol drift increases risk and reduces learning quality).
FAQ
What is “ghk cu peptide typical dosage” and how should I use it?
“Typical dosage” usually refers to the community’s commonly reported microgram ranges. I treat it as a starting reference for planning, not as a direct prescription—then I convert to the correct dosing volume using your specific reconstitution concentration and your defined schedule template.
How do I calculate the right volume from a dosage chart?
Start with your desired dose in mcg, convert it to mg (mcg ÷ 1000), then divide by your solution concentration in mg/mL. Finally convert mL to µL (× 1000) if needed. This keeps your GHK-CU peptide dosage chart consistent with your vial preparation.
What should I track to know if my protocol is working or if I need changes?
Track adherence (did you follow the schedule), tolerance (any irritation or adverse reactions), and observable outcomes you care about—plus relevant confounders like skincare routine changes and sleep. I recommend reviewing at a defined checkpoint (e.g., day 14) before adjusting anything.
Conclusion
A reliable GHK-CU Peptide dosage chart isn’t about memorizing a single number—it’s about building a protocol where your concentration, dose target, and schedule all align. By converting “typical dosage” language into measurable volumes, using schedule templates, and tracking tolerance and outcomes against a defined cycle, you turn scattered guidance into something you can follow and learn from.
Next step: Choose your concentration target (mg/mL), pick a planning dose from Table A, and write your cycle schedule using Table B—then calculate your dosing volume in µL so your protocol is consistent from day one.
Discussion