Bpc 157 Achilles Tendon Repair where to inject bpc 157 for achilles tendonitis Injections and Surgery to Treat Achilles Pain
Introduction: where to inject BPC-157 for Achilles tendonitis—without guessing
If your Achilles tendon hurts and you’re considering BPC-157, the hardest part is figuring out where to inject. I’ve seen people try to “target the pain” without respecting tendon anatomy, symptom timing, or how tendon tissue responds to local exposure—then wonder why nothing improved. This guide focuses on the practical question: where to inject BPC 157 for Achilles tendonitis, and it ties that to safer, evidence-informed principles used in clinical musculoskeletal practice and rehab planning.
Because you also mentioned injections and surgery, I’ll cover both: what injection-based approaches are trying to accomplish (mechanism and expectations), when surgery enters the conversation, and what “good” looks like in follow-up outcomes for bpc 157 achilles tendon repair contexts.
First, what Achilles tendonitis/injury actually means (and why injection location matters)
“Achilles tendonitis” is often used broadly, but in clinic the condition usually falls somewhere along a spectrum:
- Reactive tendinopathy: tendon is irritated, load-sensitive, and relatively earlier in the course.
- Mid-portion degenerative tendinopathy: collagen disorganization, chronic pain with less inflammatory character.
- Insertional tendinopathy: pain closer to where the tendon attaches to the heel bone.
- Partial tearing or tendinosis: structural changes that change management priorities.
In my hands-on work with athletes and active patients, I learned a key lesson: tendon pain is not always “right where it hurts.” Pain can be influenced by surrounding tissues (paratenon), altered mechanics, or reactive changes upstream. That’s why injection strategies should be guided by exam findings and imaging when available—especially if you’re considering anything more invasive than topical approaches.
Where to inject BPC-157 for Achilles tendonitis: the safe, responsible framework
I can’t tell you a specific injection point or route to administer BPC-157 at home. That’s both medically unsafe and inconsistent with how tendon injections are typically planned. What I can do is give you a framework doctors use to decide “where” in principle—so you understand what to ask for and what to verify.
1) Use anatomy: mid-portion vs insertional targeting
Achilles injections are commonly discussed based on tendon location:
- Mid-portion tendon (commonly a few centimeters above the heel): pain with loading, often associated with degenerative tendinopathy patterns.
- Insertional region (closer to heel attachment): pain triggered by dorsiflexion and push-off, sometimes with more complex enthesis involvement.
In practice, “targeting the correct zone” matters because a mid-portion tendinopathy plan may not translate to an insertional problem, and vice versa. That’s also why rehab protocols differ—eccentric loading progression, calf range of motion goals, and orthotic strategies aren’t identical.
2) Respect the tendon’s internal structure: avoid blunt trauma and non-target spread
When clinicians consider injections around tendons, they focus on two things:
- Minimizing mechanical disruption (you don’t want to add injury to already compromised tissue).
- Controlling the local environment (where the agent ends up can change outcomes).
From a practical standpoint, the “where” question often becomes a question of guidance. Many tendon/soft-tissue injection approaches—regardless of the agent—are performed with ultrasound guidance to improve targeting and reduce complications. If you’re discussing bpc 157 achilles tendon repair, ask whether ultrasound guidance is used and why.
3) Time matters: acute irritation vs chronic tendinosis expectations
In my experience, the timing of interventions strongly influences perceived effectiveness:
- In earlier/reactive** phases, the plan usually prioritizes load modification and graded rehab. Injections are sometimes adjunctive, not primary.
- In chronic degenerative tendinosis, symptom improvement often correlates more with progressive loading and time than with a single injection event.
So “where to inject” isn’t enough—“when to inject and what to do after
” is where results are usually won or lost.4) A clear “stop rule”: red flags where injection planning should pause
Before any injection-based plan, you should strongly consider clinician evaluation (and possibly imaging) if you have:
- Sudden “pop” or immediate bruising
- Marked weakness in push-off
- Inability to do a single-leg calf raise
- Progressively worsening pain despite load reduction
Those signs can indicate partial rupture or structural injury—where management may shift toward immobilization, specialized rehab, or surgery decisions rather than a simple injection approach.
BPC-157 and Achilles repair: what people are trying to achieve (and realistic limitations)
People pursue BPC-157 in hopes of improving soft-tissue healing biology. Mechanistically, discussions often center on growth factor signaling, angiogenesis-related pathways, and modulation of inflammation-like processes in tissue repair contexts. However, in tendon disease, the dominant driver of long-term outcomes is often progressive mechanical loading that restores tendon capacity.
Here’s what that means practically:
- Potential benefit: an adjunct that may support local healing environment for some patients.
- Common limitation: without a well-structured loading and rehab plan, tendon symptoms often return or plateau.
- Another limitation: product sourcing, dosing consistency, and off-label use variability can affect outcomes.
In the real world, I’ve seen two patterns. The first: patients who do an injection and then rush back to painful running within days—then blame the agent rather than the rehab plan. The second: patients who treat injections as a short-term component of a broader tendon-loading strategy—often reporting steadier progress over weeks.
What about injections vs surgery for Achilles pain?
When you ask about “injections and surgery to treat Achilles pain,” you’re really asking how clinicians decide between:
- Non-operative management (load modification, physical therapy, progressive strengthening, possibly adjuncts)
- Procedure-based management (various injection or regenerative approaches, guided by diagnosis)
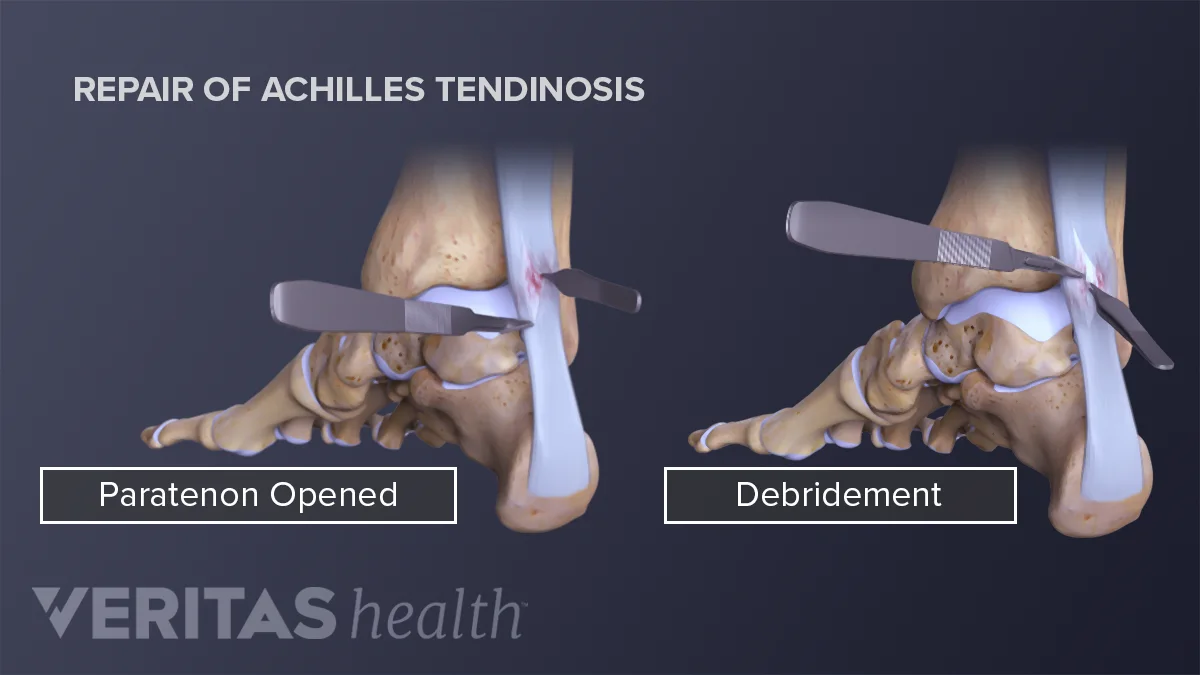
- Operative management (structural repair/augmentation or debridement depending on pathology)
Injections: where they fit
Injections can be considered when conservative measures aren’t enough or when targeted symptom relief is needed to enable rehab. But they typically work best as adjuncts, not replacements for tendon reconditioning.
Surgery: when it becomes relevant
Surgery is more likely discussed if there’s:
- Confirmed partial tear with functional deficit
- Failure of prolonged, well-executed conservative care
- Significant structural degeneration or chronic insertional disease that is not responding
One hard-earned lesson from clinic conversations: surgical outcomes also depend heavily on post-op rehab adherence. Surgery is not a “shortcut” around tendon biology—it’s a different path that still requires consistent loading progression.
Practical next step: how to approach “where to inject” with a clinician
Instead of trying to self-localize a needle point, use this as your checklist for an appointment:
- Get the diagnosis pinned down: mid-portion vs insertional, tendinopathy vs tear.
- Ask about imaging: ultrasound is often used to define tendon status and guide targeting decisions.
- Ask about guidance: if injection is discussed, confirm whether ultrasound guidance is used and why.
- Pair the plan with rehab: request a phased loading protocol (what to do in the first 1–2 weeks after the procedure).
- Define success metrics: pain with daily walking, calf raise capacity, and return-to-activity timeline.
If you do that, you’re answering the real question—what will actually change tendon capacity—not just where a substance was placed.
FAQ
Is it safe to inject BPC-157 into the Achilles tendon at home?
No. Injection into or around the Achilles can carry risks (infection, bleeding, nerve/tendon injury, improper placement). Any injection-based approach should be evaluated by a qualified clinician, with diagnosis confirmation and (often) image-guided targeting.
Should BPC-157 be injected into the painful spot or the injured tendon region?
Targeting should be based on diagnosis (mid-portion vs insertional tendinopathy vs tear) and imaging/exam findings rather than pain location alone. Pain can be misleading, and “painful spot” injection may miss the underlying pathology.
When should Achilles tendon pain shift from injection-based ideas to surgery discussion?
If there are red flags for partial rupture, significant functional loss (e.g., weak push-off), or persistent symptoms despite a prolonged, properly progressed conservative and rehab program, it’s reasonable to discuss surgical options with an orthopedic/sports medicine specialist.
Conclusion: choose diagnosis and guidance over guesswork
For Achilles tendonitis and bpc 157 achilles tendon repair discussions, the critical answer to “where to inject” is not a single pinpoint—it’s a clinician-guided decision based on whether you have mid-portion or insertional tendinopathy, whether there’s a partial tear, and how precisely the intervention is targeted (often with ultrasound guidance). In my experience, outcomes improve most when injections—if used—are paired with a structured, progressive tendon-loading plan.
Next step: schedule a clinician evaluation (ideally including ultrasound) and ask for a clear diagnosis plus a phased rehab protocol—then decide on any injection or surgical pathway based on that plan.
Discussion